
Hyperkalaemia
Introduction
Hyperkalaemia is a life threatening emergency and is one of the reversible causes of cardiac arrest.
It is usually secondary to renal failure or drugs (e.g. ACEi, K Sparing diuretics). Other causes include metabolic acidosis, rhabdomyolysis, burns, Addison’s and catabolic states e.g. sepsis, polytrauma. Pseudohyperkalaemia can occur when a blood sample haemolyzes prior to being processed.
It can be graded as mild (5.5 – 6), moderate (6-7) or severe (> 7). Severity and presence of ECG changes determine how it is treated
Clinical Features
Symptoms
Usually asymptomatic
Lethargy, muscle weakness, flacid paralysis, parasthesia
Signs
Arrhythmias causing cardiac arrest suddenly and without warning
Signs of underlying cause
Renal Failure, Fluid overload, Dehydration, Sepsis
Clinical Investigations

Bedside
VBG
Elevated Potassium level. Concurrent low pH could indicate possible renal failure causing metabolic acidosis, sepsis, hypoperfusion.
Low threshold to repeat VBG if difficult sample to obtain as haemolysis may cause pseudo hyperkalaemia
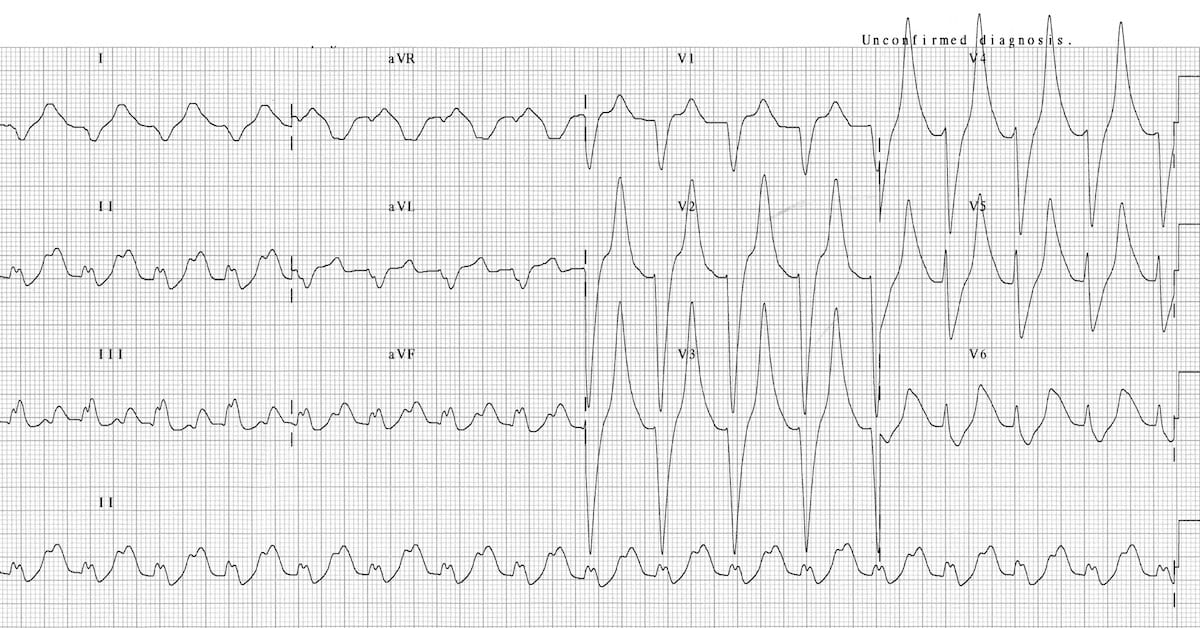
ECG Changes are characteristic and indicate severity
6-7 mmol = Tall Peake T waves (>5mm)
7-8mmol = Widening QRS, Small P waves
8-9mmol = Fusion of QRS with T wave = Sine Wave (opposite)
o > 9 mmol = AV dissociation, VT, V Fib, Asystole

Laboratory
U&E
Assess renal function. Confirm Hyper K on VBG
FBC, CRP, LFTs, blood culture if ? Sepsis
MSU

Radiology
CXR
if concerned about fluid overload or chest sepsis
Renal US
if first presentation renal failure to assess for cause
Management & Disposition
Initial Resuscitation
Patients with ECG changes should be placed on cardiac monitor
If concerned for severe hyperkalaemia patient should be managed in resus
Address ABC as clinically indicated
In the event of cardiac arrest follow hyperkalaemia ACLS algorithm
Specific Treatment (in order of priority)
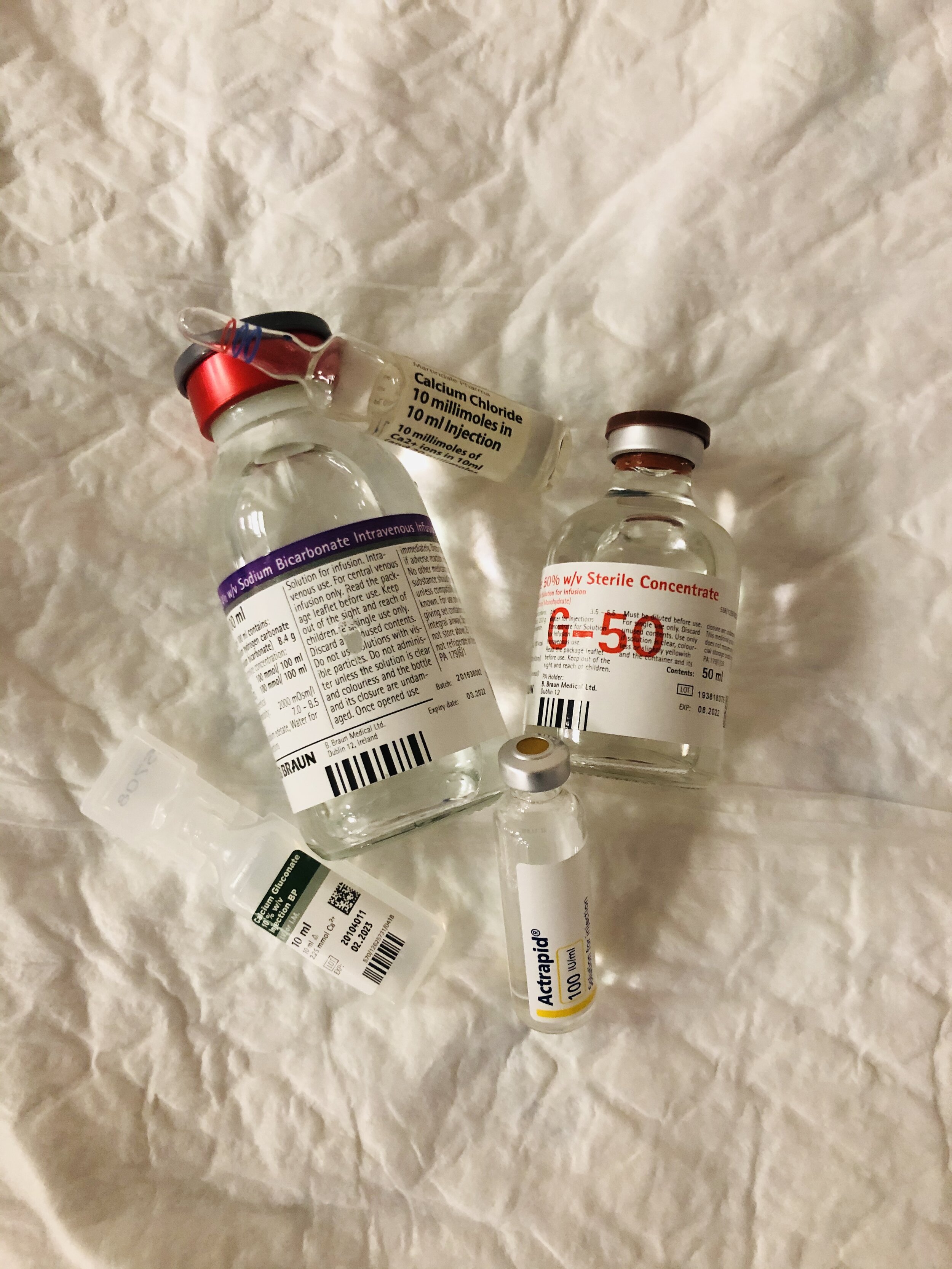
Inhibit cardiac toxicity effects of Potassium if ECG changes
10 mg IV Calcium Gluconate 10 % (stabilises the myocardium)
May be repeated. Works in minutes. Effect is temporary
Doesn’t lower potassium level
Shift Potassium into Cells
10 units IV soluble insulin (Actrapid) in 50ml Glucose 50%
Insulin causes potassium translocation. Glucose prevents associated hypoglycaemia
Nebulized Salbutamol
IV NaHCO3 infusion if concurrent severe acidosis or cardiac arrest
Enhance Potassium Secretion
Furosemide diuresis if fluid overloaded
Dialysis in those patients with ESRF
Seek and treat cause of hyperkalaemia
E.g. stop offending drugs, treat dehydration, sepsis etc
Disposition
Patients who have missed dialysis should be immediately discussed with the renal team and have dialysis arranged as a matter of urgency
Patient’s with hyperkalaemia requiring treatment i.e. > 6mmol should be admitted to hospital for treatment of hyperkalaemia and subsequent K monitoring and for work up and treatment of underlying cause
References
1. https://litfl.com/wp-content/uploads/2018/08/ECG-Hyperkalemia-serum-potassium-9.3.jpg
{kind=link}
2. Pasco J, Cameron P et al. Chapter 12.2 Electrolyte Disturbance. Adult Textbook of Emergency Medicine. 4th Edition
This blog was written by Dr Deirdre Glynn and was last updated in December 2020